BPC-157: mechanism, evidence, and what the research actually shows
BPC-157 is the most-searched healing peptide. Here's the mechanism, the preclinical evidence, the limited human data, and how to think about the protocol.

BPC-157 is the most-searched non-weight-loss peptide in the world. The preclinical evidence is broad and consistent: accelerated tendon repair, enhanced angiogenesis, faster wound healing, and anti-inflammatory effects across multiple injury models. The human clinical evidence is thin by comparison. Understanding BPC-157 means holding both facts at once.
What BPC-157 is#
BPC-157 stands for Body Protection Compound 157. It's a synthetic 15-amino-acid peptide fragment originally isolated from a larger protective protein found in human gastric juice. The native protein's role is to help maintain gastric mucosal integrity; the 15-residue fragment retains biological activity and is dramatically more stable than the full-length parent molecule.
BPC-157 is administered subcutaneously or intramuscularly. Oral preparations exist but the pharmacokinetics differ substantially — oral BPC-157 acts primarily on the gastrointestinal tract itself rather than distributing systemically. For musculoskeletal indications, the injected form is what the preclinical literature was built on.
The preclinical mechanism#
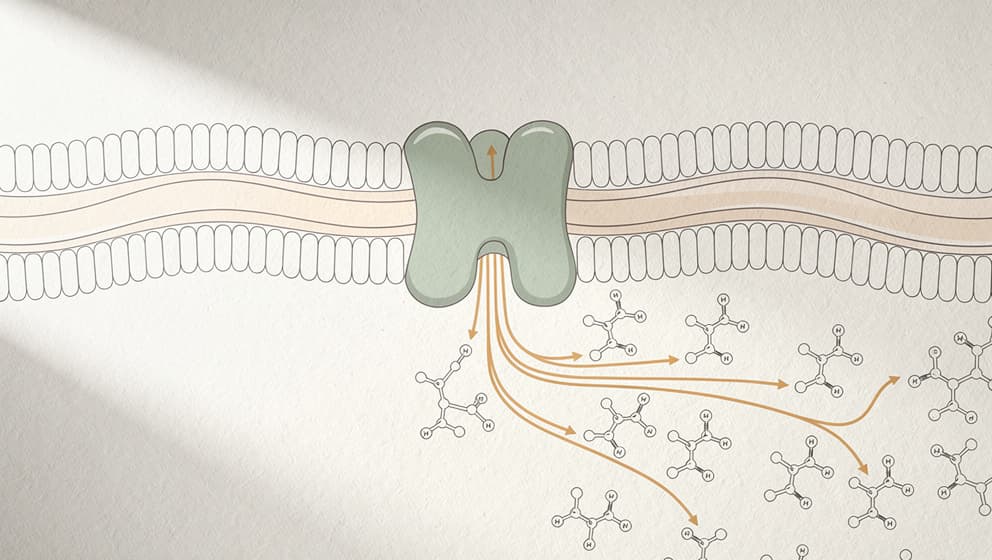
BPC-157 activates several overlapping pathways relevant to tissue repair. Recent systematic reviews consolidate the mechanism around four primary effects:
1. Angiogenesis via VEGFR2 and Akt-eNOS signalling. BPC-157 upregulates vascular endothelial growth factor receptor 2 (VEGFR2) and activates the Akt-endothelial nitric oxide synthase pathway, promoting new blood vessel formation at injury sites. More blood supply means more oxygen and nutrients to healing tissue.
2. Fibroblast migration and survival. In tendon fibroblast cell lines, BPC-157 dramatically increases phosphorylation of FAK (focal adhesion kinase) and paxillin, leading to more cell migration and survival at injury sites. This is the mechanism behind the tendon-healing results in animal models.
3. Anti-inflammatory modulation. BPC-157 reduces production of pro-inflammatory cytokines (IL-6, TNF-alpha) in multiple injury models, without suppressing immune function broadly.
4. Growth-hormone receptor upregulation. Preclinical studies show BPC-157 increases growth-hormone receptor expression on tendon fibroblasts, which may explain synergistic effects when BPC-157 is stacked with GH-releasing peptides.
Preclinical evidence base#

The preclinical evidence for BPC-157 is unusually consistent. Systematic reviews covering dozens of animal studies describe improved outcomes across tendon, ligament, muscle, bone, and mucosal injury models:
- Tendon: accelerated collagen deposition, improved biomechanical strength, reduced healing time
- Ligament: improved structural integrity in anterior cruciate ligament models
- Muscle: faster recovery from traumatic injury in rat models
- Bone: enhanced fracture healing
- Gastric and intestinal mucosa: protection against NSAID-induced ulceration, accelerated ulcer healing
- Tendon-to-bone healing: improved integration in rotator-cuff repair models
The pattern is that BPC-157 shows effects across multiple tissue types and injury mechanisms in preclinical work. Whether those effects translate to clinically meaningful human outcomes is the open question.
Human clinical evidence is limited#
As of 2025, three pilot human studies have been published:
- Intra-articular knee pain — a small open-label pilot in adults with knee osteoarthritis.
- Interstitial cystitis — a small study examining BPC-157 for chronic bladder inflammation.
- Intravenous safety and pharmacokinetics (Lee and Burgess, 2025) — two healthy adults received intravenous BPC-157 infusions up to 20 mg. Well tolerated, no adverse effects, plasma levels returned to baseline within 24 hours.
All three were small, open-label, and exploratory. No large randomised controlled trial exists as of April 2026.
That's not the same as "no evidence" — the preclinical base is substantial. It's also not the same as established clinical efficacy. The honest framing: BPC-157 has a biologically plausible mechanism, strong preclinical support, and limited human outcome data.
Dosing and administration#
Research-use BPC-157 protocols have coalesced around a standard range from applied musculoskeletal research:
- Typical dose: 250–500 mcg per injection
- Frequency: once or twice daily
- Route: subcutaneous injection, preferably near the injury site
- Duration: typical research-use cycles run 4–8 weeks, with longer cycles for chronic conditions
Reconstitution math: a 5 mg BPC-157 vial reconstituted with 2 mL of bacteriostatic water gives 2,500 mcg/mL. A 250 mcg dose equals 10 syringe units on a standard 1 mL insulin syringe. A 500 mcg dose equals 20 units. The Klarovel peptide calculator handles any vial size and target dose.
Proximity matters in preclinical data. Injection near the injury site appears to produce better outcomes than systemic injection in most animal studies, though the pharmacokinetics of this effect in humans are not well characterised. Practical implication: for a knee injury, subcutaneous injection in the adjacent soft tissue; for an Achilles tendon, nearby calf tissue.
Side effects and safety#
BPC-157's safety profile in preclinical and the limited human data is benign:
- No serious adverse events reported in any of the three human pilot studies
- No meaningful toxicity in long-term rat studies at doses far above human equivalent
- No reported drug interactions of clinical significance
The most common reported side effects are mild and transient: injection-site irritation, brief lightheadedness, nausea in a small percentage of users. These are common across all subcutaneous peptides and are not specific to BPC-157.
Regulatory status#
BPC-157 is not approved as a medicine in the United States, the European Union, or Norway. Legemiddelverket has not authorised BPC-157 for any indication. In practice:
- It is legally classified as a research compound in most jurisdictions.
- It is not available through pharmacies.
- It is distributed through specialised research-peptide suppliers, including Klarovel's catalogue, which stocks BPC-157 in both pen and vial formats.
- Anyone considering use should understand the distinction between research-use and medical prescription, and should screen for contraindications before starting.
BPC-157 in practice#
Three realistic scenarios where BPC-157 is commonly researched:
Tendon/ligament injury recovery. This is the best-supported indication in animal models. Typical protocols run 4–8 weeks with subcutaneous injection near the injury site, 250–500 mcg twice daily during acute phase, tapering to once daily during maintenance.
Gastrointestinal conditions. Preclinical evidence is strong for mucosal healing. For GI-specific goals, oral preparations have their own rationale (local effect), though injected forms also show systemic anti-inflammatory effects.
Stacking with TB-500. Many research protocols combine BPC-157 with TB-500 (thymosin beta-4 fragment) for broader tissue-repair coverage. The evidence for the stack is less established than for either peptide individually. See the BPC-157 + TB-500 stack guide.
The one-sentence summary#
BPC-157 has a strong preclinical mechanism, limited human data, a benign short-term safety profile, and no regulatory approval. It's not a guaranteed fix. It's a biologically plausible option for well-screened research-use applications, particularly in musculoskeletal recovery where the preclinical literature is deepest.
For anyone considering a BPC-157 protocol, the right starting point is Klarovel's questionnaire — which screens for contraindications, maps against the engine's peptide catalogue, and produces a protocol with structured bloodwork and dose recommendations. The reconstitution guide covers the mechanics. The peptide calculator handles the dose math.
BPC-157 is the peptide that earns its reputation when protocol discipline matches the preclinical promise. Without the discipline, it's just an injection.
Keep reading
Selank Peptide: Russian-Approved, Not FDA-Authorized
Selank peptide is a Russian-approved anxiolytic that modulates GABA-A and enkephalins. The mechanism, the 62-patient trial, and 2026 regulatory reality.
Semax Peptide: Approved in Russia, Unscheduled in the US
Semax peptide is a Russian-approved nootropic that raises BDNF and shows neuroprotective effects after stroke. The science and the 2026 regulatory reality.
Cognitive peptides: promise, evidence, and a retraction
Research-first walkthrough of cognitive peptides, what Semax, Selank, and DSIP actually do, which claims don't hold up, and what to watch in 2026.