Selank Peptide: Russian-Approved, Not FDA-Authorized
Selank peptide is a Russian-approved anxiolytic that modulates GABA-A and enkephalins. The mechanism, the 62-patient trial, and 2026 regulatory reality.
Russia approved Selank peptide in 2009 for generalized anxiety disorder and neurasthenia, on the strength of a small but well-designed comparison against medazepam, a long-running Soviet-era benzodiazepine. Seventeen years later, the FDA, the EMA, and Norway's Legemiddelverket have authorized none of it. The interesting part is that the Russian trial did not just match the benzodiazepine; it produced effects benzodiazepines cannot produce. That is where the honest conversation about Selank peptide has to start.
Selank peptide is a tuftsin-derived heptapeptide approved for anxiety in Russia and unlicensed everywhere else#
The active sequence is Thr-Lys-Pro-Arg-Pro-Gly-Pro: four residues that match tuftsin, an immunoregulatory tetrapeptide naturally cleaved from immunoglobulin G, plus the same Pro-Gly-Pro stabilizing tail used in Semax (Pavlov et al., PubMed 30255741). The native tuftsin fragment was rapidly cleaved by serum and brain peptidases. Adding Pro-Gly-Pro stretches the functional window enough for the peptide to reach receptors before degradation, even though the parent molecule still clears from plasma in about 25 minutes.
Russia approved Selank for clinical use in 2009 for two indications: generalized anxiety disorder (GAD) and neurasthenia, the latter being a Russian-specific diagnostic category that overlaps with what Western medicine would call chronic functional fatigue with anxiety overlay. The approval rested on a multi-year clinical program at the Russian Institute of Molecular Genetics, with the most-cited trial being Zozulya et al., 2008 (PubMed 18454096), a comparison against medazepam in 62 patients. Approval came shortly after.
Outside Russia and Ukraine, the regulatory picture is empty. The US FDA has not approved Selank. The EMA has not authorized it. Norway's Legemiddelverket has no marketing-authorization record. The clinical evidence package that satisfied Russian regulators in the 2000s was never submitted to Western agencies, and the original patent expired before a Western firm had reason to fund the multi-hundred-million-dollar trials approval would now require. Generic competitors would arrive the day approval did.
This is the same regulatory contradiction that defines Semax peptide, Selank's cognitive sister-compound from the same institute. Both have decades of Russian clinical use, real mechanism evidence, and zero approvals where it matters legally for Norwegian residents.
Selank peptide modulates GABA-A receptors as a subtype-selective allosteric agent, not a benzodiazepine substitute#
The mechanism is more interesting than "tuftsin analogue with anxiolytic effect" suggests. Research has shown Selank affects GABA-A receptor function as a positive allosteric modulator with subtype selectivity, distinct from the benzodiazepine binding site (Pavlov et al., PubMed 30255741). In receptor assays the relationship runs in both directions: Selank can block the modulatory activity of diazepam at GABA-A, suggesting overlapping but non-identical binding sites.
A 2016 study put numbers on the gene-expression cascade. Volkova and colleagues administered intranasal Selank at 300 µg/kg to rats and measured GABA-A subunit mRNA expression in the frontal cortex at one and three hours (PMC 4757669). At one hour, Selank produced a 1.58-fold increase in Gabrb3 expression with concomitant decreases in Gabre and Gabrq. At three hours, the picture inverted: Gabre rose 16-fold and Gabrq rose 13-fold from baseline. The gene-transport machinery (Slc32a1, Slc6a1, Slc6a11) showed similar bidirectional shifts. Whatever Selank is doing at the receptor level, it is not a single static effect. The system reorganizes over hours.
A second mechanism involves the enkephalin system, which is one reason the Selank GABA story does not fully explain the clinical picture. Patients with GAD show reduced leu-enkephalin levels that correlate with anxiety severity. Selank administration was associated with restored enkephalin levels, and the magnitude of restoration correlated with anxiety reduction (Zozulya et al., PubMed 18454096). This places Selank inside two parallel anti-anxiety systems at once: the GABAergic one shared with benzodiazepines, and the opioidergic one that classical anxiolytics do not touch.
Preclinical work also reports BDNF upregulation downstream of Selank, similar to but smaller in magnitude than what Semax produces. The cognitive side of Selank's clinical profile (sharper attention, cleaner working memory on dosing days) plausibly reflects this BDNF effect rather than a stimulant action.
Selank vs benzodiazepine: a 62-patient Russian trial showed equivalent anxiolysis to medazepam plus antiasthenic effects benzodiazepines never produce#
The clinical signal that earned Selank Russian regulatory approval came from Zozulya, Neznamov, and colleagues, 2008 (PubMed 18454096), published in Zhurnal Nevrologii i Psikhiatrii imeni S.S. Korsakova. Sixty-two patients with GAD or neurasthenia were randomized: 30 to Selank, 32 to medazepam (a Russian-formulary benzodiazepine with a long anxiolytic record). Both arms received 14 days of treatment.
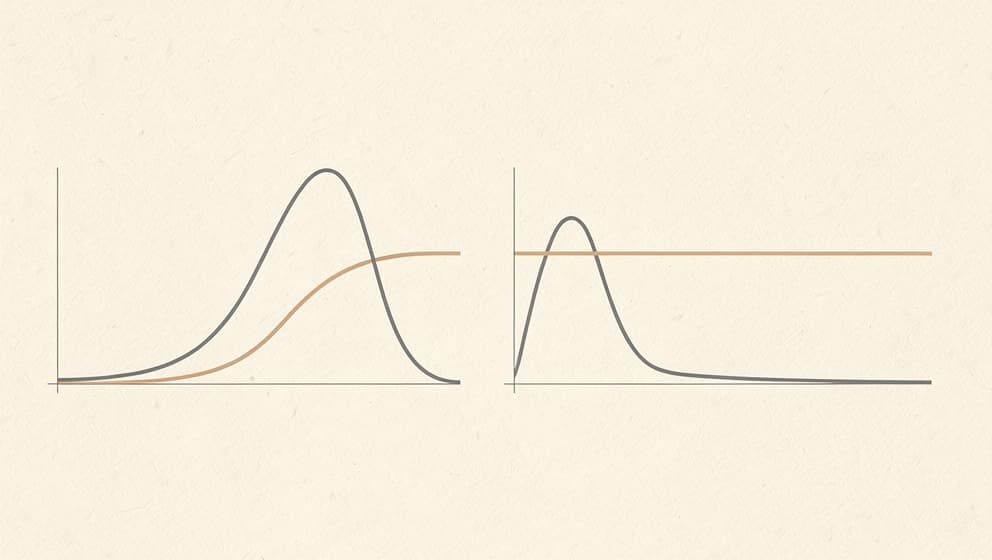
Anxiolytic efficacy on the Hamilton Anxiety Rating Scale (HARS) was statistically equivalent between arms. Studies have shown roughly 40% of patients in either arm met criteria for "rapid response" with HARS scores dropping abruptly by day 3 of treatment, with a representative trajectory of 20.3 down to 7.0. The other 60% showed slower but eventually comparable response curves.
What the Selank arm produced that the medazepam arm did not was a pair of secondary effects: antiasthenic activity (reduction in fatigue, improved daytime function) and a mild psychostimulant signal (sharper attention, faster reaction times). Benzodiazepines tend to produce the opposite: sedation, reaction-time slowing, and cognitive dulling that show up reliably on Stroop or n-back testing. Selank patients did not show these signatures. The clinical implication, restated cautiously: Selank may support anxiety relief without the cognitive cost benzodiazepines impose.
A second supporting line of evidence comes from preclinical work. In a chronic mild stress rat model, Selank administered alone reduced elevated anxiety more effectively than diazepam alone, with the combination Selank + diazepam producing intermediate effects (Kasian et al., PubMed 28280289). The result is unusual. Adding a known anxiolytic to another should reinforce, not dilute, but the combination here did not exceed Selank monotherapy. This is consistent with the receptor-binding observation that Selank can interfere with diazepam's modulatory activity at GABA-A.
What the published Western literature does not show is a Phase 3 randomized controlled trial. The Russian dataset is small-trial single-center, language-bound, and not powered the way modern psychiatric drug trials are powered. Until those trials exist, Selank's clinical claim rests on a coherent but not bulletproof body of work.
The pharmacokinetic profile favors intranasal delivery: high bioavailability and CNS uptake within seconds#
Selank's pharmacokinetics shape how it is dosed. The standard parent peptide has a plasma half-life of roughly 25 minutes, longer than Semax's two-to-five-minute window but still short by small-molecule drug standards. The behavioral effect outlasts the plasma curve by several hours, suggesting that the receptor and gene-expression effects propagate after the peptide itself is cleared.
Intranasal Selank is the dominant route in the Russian clinical literature, and the pharmacokinetic reasoning is straightforward. Bioavailability via the nasal mucosa is high; CNS uptake is fast through the olfactory and trigeminal pathways; first-pass metabolism is bypassed. Subcutaneous Selank produces comparable systemic exposure but loses the direct nose-to-brain access. The Russian protocols accordingly favor intranasal dosing, with the most-cited research range sitting at 250 to 1000 mcg per administration, one to three times daily, for 10-to-14-day cycles.
For practical math on intranasal versus subcutaneous formulations, Klarovel's reconstitution calculator walks through the mcg-to-unit conversion per vial concentration. The PK profile does not mean Selank intranasal dosing is interchangeable with subcutaneous; it means the route matters as much as the dose, and the published clinical evidence is intranasal-heavy.
The reported side-effect profile is unusually narrow for an anxiolytic, but unlicensed sourcing introduces real quality risk#
Selank's safety record across roughly two decades of Russian clinical use has stayed remarkably narrow. The published Selank side effects literature does not show sedation, dependence, withdrawal, or rebound anxiety on discontinuation. The most common acute issues are nasal irritation in intranasal users (route-dependent, similar to Semax), mild headache, and occasional sleep disruption when dosed too late in the day. Mild nausea is reported by a minority. None of these have produced organ toxicity, hepatic concerns, or cardiac signals in the Russian post-marketing surveillance.
For an anxiolytic, this is unusual. Benzodiazepines produce dependence in roughly 20-30% of long-term users, withdrawal in a higher fraction on rapid taper, and cognitive impairment that compounds across years of use. Selank produces none of those signatures across the published record. The honest caveat is that the published record is also smaller than the benzodiazepine record, and absence of evidence is not evidence of absence; rare adverse events that affect 1-in-10,000 patients are easy to miss in trials of fewer than 100.
The Norwegian dimension of source-quality risk is concrete. The Norwegian Directorate of Health adjacent youth-advisory service ung.no addressed Selank specifically, telling a young inquirer that Selank and Semax are not approved medicines in the EU or Norway, that buying peptides online is "in itself dangerous," and that the practical answer is "no, it is not worth it." This is a Norwegian-language primary voice on the question, not a Klarovel framing.
Selank peptide has no Norwegian marketing authorization, and Legemiddelverket treats it as an unlicensed peptide#
In Norway, Selank sits in the same legal architecture as every other peptide without a Norwegian marketing authorization. Legemiddelverket has not registered Selank as a medicinal product, the EMA has not authorized it, and that places Selank under forskrift 2004-11-02-1441 § 3-2, which prohibits postal import of medicines, prescription or over-the-counter, into Norway. Tolletaten enforces this at customs by seizing and destroying packages.
The 2025 addition of BPC-157 to the Norwegian Medicines Agency's named stop-list set the precedent that the agency will explicitly call out specific compounds when import volume warrants action. Selank is not currently named in the same way, but the underlying legal framework is identical. Buying Selank from a research-chemistry supplier and shipping it to a Norwegian address falls inside the same forskrift, with the same enforcement at customs, regardless of how the package is labeled.
For Norwegian readers researching the cognitive-anxiety peptide class, the practical conclusion mirrors the one in Klarovel's guide on the legal status of peptides in Norway: the current 2026 framework leaves no compliant import route for Selank. The path forward is either a Norwegian-licensed alternative (where one exists for a given indication, which for anxiety means standard prescription anxiolytics), or no peptide at all.
Frequently asked questions about Selank peptide#
Is Selank peptide legal in Norway? Selank is not registered as a medicinal product in Norway. Legemiddelverket has no marketing authorisation on file for it, and Tolletaten enforces forskrift 2004-11-02-1441 § 3-2 by seizing peptide imports at customs. The Norwegian youth-advisory service ung.no has been explicit on this point, telling young inquirers that Selank is not approved in the EU or Norway and that buying peptides online is unsafe.
How does Selank peptide compare to benzodiazepines like alprazolam or diazepam? Selank produces equivalent anxiolytic effect on standardized scales (Hamilton Anxiety Rating Scale) in the published Russian literature, but without the sedation, cognitive dulling, dependence, or rebound that define the benzodiazepine class. The mechanism is also distinct: Selank acts as a subtype-selective allosteric modulator of the GABA-A receptor at a site separate from where benzodiazepines bind. Research suggests Selank can even block diazepam's modulatory activity at GABA-A, which is why combining the two does not produce additive anxiolysis.
Can Selank and Semax be stacked? Russian protocols sometimes pair the two, with Semax providing focus enhancement and Selank providing anxiolysis. The mechanisms are non-overlapping: Selank works primarily through GABA-A and enkephalins, while Semax works primarily through BDNF and TrkB signalling. There is no published Western RCT on the combination. Klarovel's protocol engine handles stacking compatibility automatically based on questionnaire data and known mechanism overlap; the standard caution is that combining peptides multiplies the side-effect surface even when each is well tolerated alone.
How fast does Selank peptide work? Some users report acute anxiety reduction within 30 to 90 minutes of an intranasal dose. The Russian clinical trial data indicate that roughly 40% of patients qualify as "rapid responders" with HARS scores dropping abruptly within the first three days of treatment. The remaining 60% show a slower response curve over the typical 14-day course. The neurotrophic and gene-expression effects operate on a slower timescale and may continue to develop over weeks of consistent dosing.
Is intranasal or subcutaneous Selank better? The Russian clinical literature is built almost entirely on the intranasal route, which bypasses first-pass metabolism and provides direct nose-to-brain delivery through the olfactory and trigeminal systems. Subcutaneous Selank achieves comparable systemic exposure but loses the direct CNS access and is less well-characterized in the published trials. For research-protocol use, intranasal dosing has the deeper evidence base.
Where Selank peptide fits in Klarovel's broader cognitive peptide framework#
The honest framing for Selank peptide is the one that opened this guide: a compound with two decades of Russian clinical use as an anxiolytic that may support anxiety relief without the cognitive cost benzodiazepines impose, real mechanism evidence at GABA-A and the enkephalin system, and zero approvals in the regulatory frameworks that govern Norwegian residents. None of those facts cancel each other out. The Russian psychiatric literature is genuine. The Western evidence gap is also genuine. Both are true at once, and any guide that pretends otherwise is simplifying.
For readers building a clearer picture of where Selank peptide fits relative to Semax, DSIP, and Cerebrolysin, the cognitive peptides pillar is the next stop. For readers wanting to understand which peptide class might align with their specific bloodwork, goals, and constraints, the Klarovel questionnaire is the route through. Complete the Klarovel questionnaire to see what the engine recommends based on a full health profile rather than a single compound's reputation.
Keep reading
Semax Peptide: Approved in Russia, Unscheduled in the US
Semax peptide is a Russian-approved nootropic that raises BDNF and shows neuroprotective effects after stroke. The science and the 2026 regulatory reality.
Cognitive peptides: promise, evidence, and a retraction
Research-first walkthrough of cognitive peptides, what Semax, Selank, and DSIP actually do, which claims don't hold up, and what to watch in 2026.

BPC-157: mechanism, evidence, and what the research actually shows
BPC-157 is the most-searched healing peptide. Here's the mechanism, the preclinical evidence, the limited human data, and how to think about the protocol.