CJC-1295 + Ipamorelin: the GH synergy stack explained
The CJC-1295 + Ipamorelin stack pairs a GHRH analogue with a GHRP for amplified growth hormone pulses. Here's the mechanism, the dose pattern, and what the research shows.
The CJC-1295 + Ipamorelin stack is the canonical growth-hormone-axis peptide combination. Pairing a GHRH analogue (CJC-1295) with a GHRP (Ipamorelin) produces amplified endogenous growth hormone pulses — larger than either peptide alone, with a cleaner side-effect profile than higher-potency GHRPs. Understanding why the stack works requires understanding the GH axis.
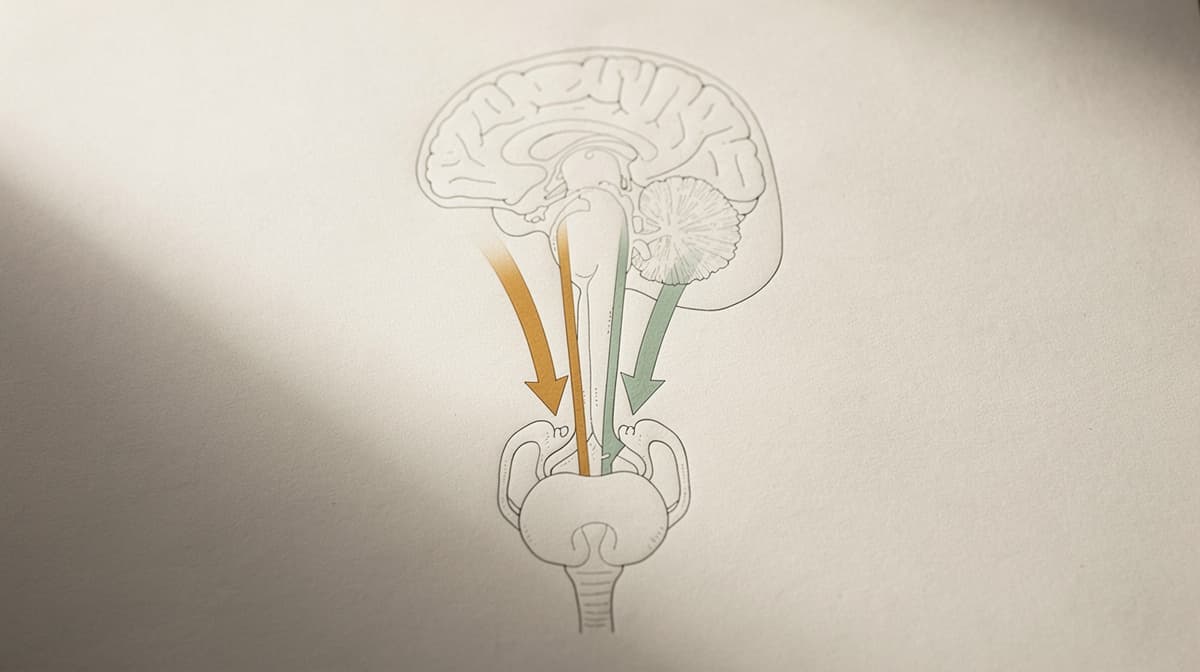
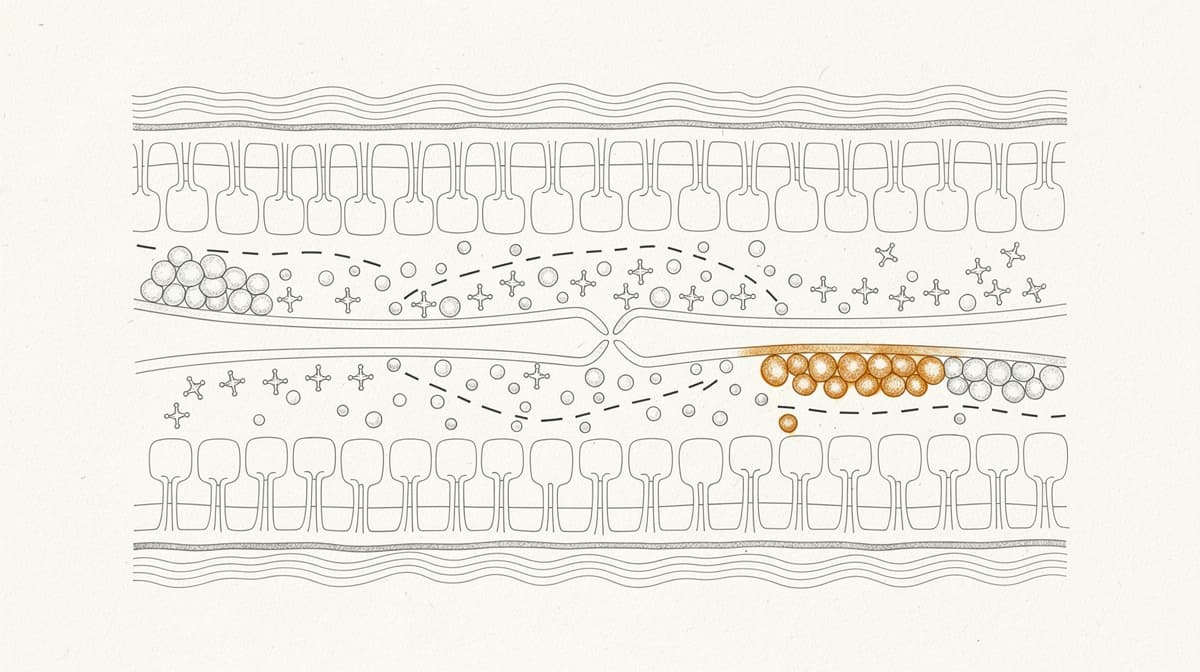
The growth hormone axis in one diagram#
Endogenous growth hormone is released in pulses throughout the day, with the largest pulse during early night sleep. The pulses are controlled by two opposing hypothalamic hormones:
- GHRH (growth hormone releasing hormone) — stimulates GH release from the anterior pituitary
- Somatostatin — inhibits GH release
Ghrelin, secreted by the stomach, also stimulates GH release through a separate receptor (GHS-R) on the same pituitary cells. It's a parallel activation path.
Therapeutic peptides in the GH axis fall into three categories:
- GHRH analogues: CJC-1295 (no DAC and DAC forms), Sermorelin, Tesamorelin
- GHRPs (ghrelin mimetics): Ipamorelin, GHRP-2, GHRP-6, Hexarelin
- Oral non-peptide: MK-677 (ibutamoren)
The CJC-1295 + Ipamorelin stack combines categories 1 and 2. The two peptides activate different receptors on the same pituitary cells, producing a larger GH pulse than either alone.
Why the stack produces synergy#
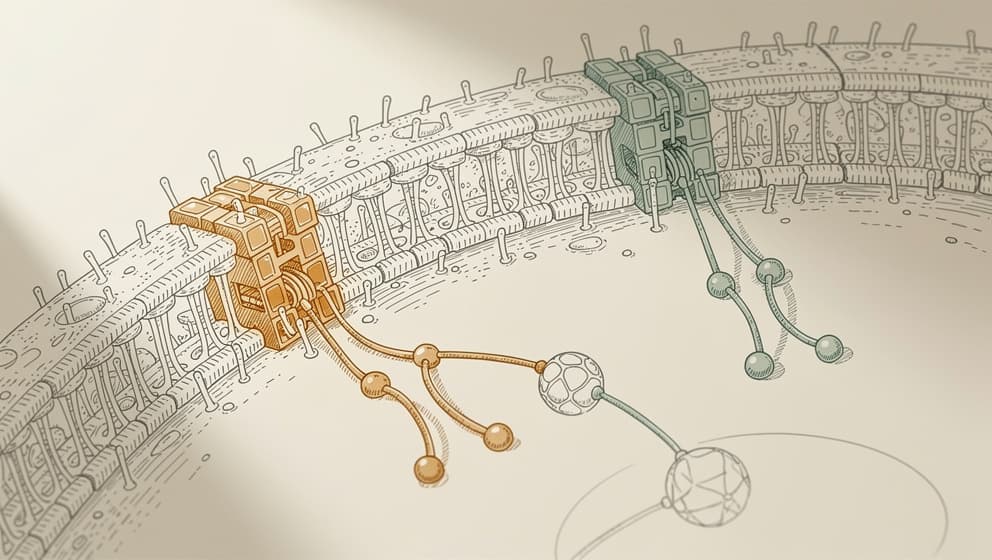
The synergy is pharmacological, not marketing. A GHRH analogue alone (CJC-1295) amplifies the pituitary's response to GH-releasing signals. A GHRP alone (Ipamorelin) directly triggers GH release. Combining them hits both receptor systems simultaneously — and the two signals converge on the same downstream machinery, producing a larger pulse of GH than either mechanism activated alone.
In preclinical and applied-research data, the combined GH pulse is roughly 3–5× larger than from either peptide alone at comparable doses. That's the mechanism reason the stack is so commonly used in research-use GH protocols.
Ipamorelin specifically is chosen over other GHRPs because it has the cleanest side-effect profile. Unlike GHRP-2 and GHRP-6, Ipamorelin does not meaningfully elevate cortisol or prolactin. That matters because cortisol elevation counteracts some of the anabolic effects of GH, and prolactin elevation is undesirable for almost all use cases.
Dosing and administration#

Typical research-use protocol:
- CJC-1295 (no DAC): 100 mcg per injection
- Ipamorelin: 200 mcg per injection
- Frequency: 1–3× daily
- Timing: ideally 30–60 minutes before bed (to match natural GH pulse); morning-fasted and pre-workout doses are common additions
- Route: subcutaneous
- Cycle length: 8–12 weeks on, 4 weeks off
The daily frequency depends on intensity. Beginners or protocols focused on sleep and recovery often use 1× nightly. More aggressive protocols use 3× daily (morning-fasted, pre-workout, pre-bed) to generate three amplified GH pulses.
Reconstitution for Klarovel's blend product (5 mg CJC + 10 mg Ipamorelin per pen, or 5 mg + 5 mg vial): see the peptide calculator for exact syringe units based on your chosen reconstitution volume.
CJC-1295 no DAC vs DAC: the difference is half-life. The "DAC" form has a C-terminal modification that extends the half-life to roughly 6–8 days (versus ~30 minutes for no DAC). The DAC form produces sustained GHRH stimulation rather than pulsatile stimulation — which is a different biological signal. Most stack protocols use the no DAC form because pulsatile GH release is closer to natural physiology and avoids chronic receptor desensitisation. The DAC form is used in protocols where pulsatility isn't required.
Expected effects and timeline#
The GH axis responds over weeks, not days. Typical research-reported timeline:
- Weeks 1–2: improved sleep quality (deeper, more restorative)
- Weeks 3–4: more pronounced recovery from training, gradual fat-mass reduction
- Weeks 5–8: body composition shifts become measurable — moderate fat-mass reduction, slight lean-mass preservation or gain
- Weeks 9–12: peak effects, with IGF-1 levels typically in the upper half of the age-adjusted reference range
- Post-cycle: effects fade over 4–8 weeks unless maintained
IGF-1 monitoring is non-negotiable. Growth-hormone-axis protocols require baseline IGF-1, a repeat measurement at 4–6 weeks, and a final measurement at cycle end. If IGF-1 rises above the age-adjusted reference range, dose reduction or cycle pause is indicated. Klarovel's questionnaire builds bloodwork schedules into the protocol automatically.
Side effects and safety#
The stack's side-effect profile is mild compared to other GH-axis protocols:
- Transient water retention (first 1–2 weeks)
- Mild injection-site irritation
- Brief fatigue after large evening doses (if dosed too late)
- Increased hunger from ghrelin mimicry (noticeable with higher Ipamorelin doses)
- Tingling or numbness in extremities at higher doses (Ipamorelin-driven)
Cortisol and prolactin elevations that occur with GHRP-2 and GHRP-6 are not meaningful with Ipamorelin. Glucose and insulin sensitivity changes are minimal at typical research doses but worth monitoring over long cycles.
Regulatory status and access#
Neither CJC-1295 (no DAC or DAC) nor Ipamorelin is approved as a medicine in the US, EU, or Norway. Legemiddelverket has not authorised either compound. Both are classified as research peptides.
Klarovel stocks the combination product in:
- Pen format: 5 mg CJC-1295 + 10 mg Ipamorelin per pen
- Vial format: 5 mg CJC-1295 + 5 mg Ipamorelin per vial
The pen format simplifies dosing at the cost of fixed ratios; the vial format allows for separate dosing if the protocol calls for different CJC-to-Ipamorelin ratios.
The realistic expectation#
The CJC-1295 + Ipamorelin stack is the most-researched and most-used GH-axis protocol for a reason. The mechanism is sound, the side-effect profile is benign, and the effects — improved sleep, gradual fat-mass reduction, faster recovery — are noticeable within 4–8 weeks for most well-screened users.
It is not an anabolic-steroid replacement. GH-axis effects are subtle compared to direct anabolic-androgen use. It is not a shortcut for underlying lifestyle issues — protocols that produce best effects are layered on adequate sleep, consistent training, and baseline bloodwork.
For protocol planning, Klarovel's questionnaire handles screening and bloodwork requirements. The peptide calculator handles reconstitution math. The Ipamorelin guide covers the GHRP mechanism in depth.
CJC-1295 + Ipamorelin is the cleanest, most-studied GH-axis protocol in the research-use catalogue. The stack is as good as the foundation underneath it. Get the screening right, run the IGF-1 bloodwork, and the rest follows.
Keep reading
Selank Peptide: Russian-Approved, Not FDA-Authorized
Selank peptide is a Russian-approved anxiolytic that modulates GABA-A and enkephalins. The mechanism, the 62-patient trial, and 2026 regulatory reality.
Semax Peptide: Approved in Russia, Unscheduled in the US
Semax peptide is a Russian-approved nootropic that raises BDNF and shows neuroprotective effects after stroke. The science and the 2026 regulatory reality.
Cognitive peptides: promise, evidence, and a retraction
Research-first walkthrough of cognitive peptides, what Semax, Selank, and DSIP actually do, which claims don't hold up, and what to watch in 2026.