Ipamorelin: the cleanest GHRP in the research catalogue
Ipamorelin is the most selective ghrelin mimetic in the GHRP class. No meaningful cortisol or prolactin elevation. Here's the mechanism, dose framework, and evidence.

Ipamorelin is the cleanest growth-hormone-releasing peptide (GHRP) in the research catalogue. Where GHRP-2 and GHRP-6 trigger GH release but also elevate cortisol, prolactin, and appetite, Ipamorelin triggers GH release selectively. That's why it's the default GHRP in modern stack protocols.
What Ipamorelin is#
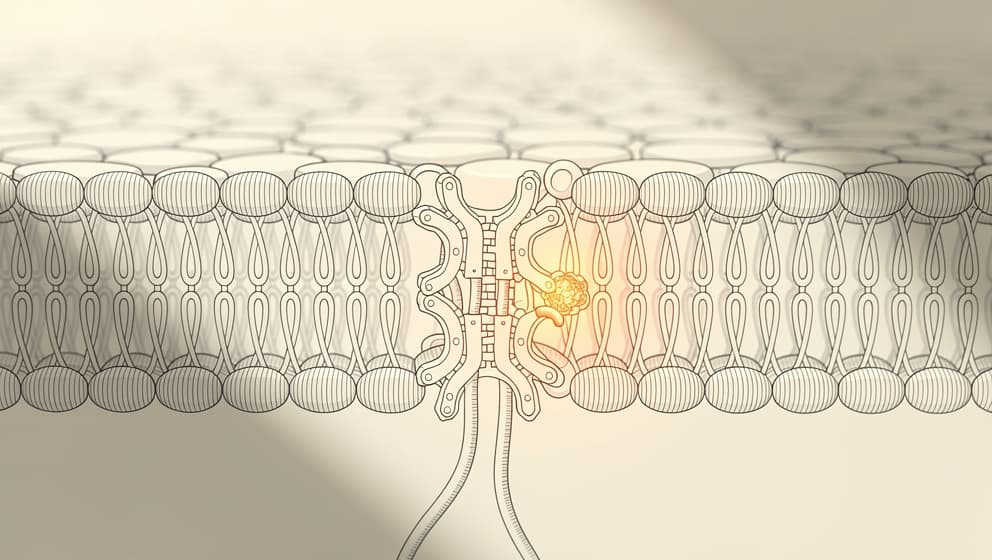
Ipamorelin is a synthetic pentapeptide (five amino acids) that binds to the growth hormone secretagogue receptor (GHS-R, also called the ghrelin receptor). Activating GHS-R triggers growth hormone release from the anterior pituitary — the same pathway the stomach hormone ghrelin uses.
What makes Ipamorelin distinctive among GHRPs is selectivity. Other GHRPs (GHRP-2, GHRP-6, Hexarelin) activate GHS-R but also have affinity for receptors that drive cortisol release, prolactin elevation, and aggressive appetite stimulation. Ipamorelin has near-zero affinity for those off-target receptors at typical doses.
That selectivity matters. Cortisol elevation counteracts some of the anabolic and recovery effects of GH. Prolactin elevation is undesirable for virtually all use cases. Aggressive appetite stimulation from GHRP-6 can undermine body-composition goals. Ipamorelin avoids all three.
The mechanism in context#
The GH axis has two activation paths:
- GHRH pathway — hypothalamic GHRH activates pituitary GHRH receptors, triggering GH release (CJC-1295, Sermorelin, Tesamorelin act here)
- GHS-R / ghrelin pathway — stomach ghrelin or synthetic GHRPs activate GHS-R, also triggering GH release (Ipamorelin, GHRP-2, GHRP-6, MK-677 act here)
Both pathways converge on the same GH-producing cells. Activating both simultaneously produces larger GH pulses than either alone. That's why Ipamorelin is typically paired with a GHRH analogue — see CJC-1295 + Ipamorelin stack.
Dosing and administration#

Standard research-use dosing:
- Dose: 200 mcg per injection
- Frequency: 1–3× daily
- Route: subcutaneous
- Timing: morning fasted, pre-workout, and/or 30–60 minutes before bed
- Cycle length: 8–12 weeks on, 4 weeks off
Reconstitution math: a 10 mg Ipamorelin vial + 2 mL BAC water = 5,000 mcg/mL. A 200 mcg dose = 4 syringe units on a standard insulin syringe. The peptide calculator handles any vial size.
Single peptide or stacked? Ipamorelin alone produces GH pulses but at lower amplitude than the CJC-1295 + Ipamorelin combination. For protocols that prioritise simplicity or lower-cost entry points, Ipamorelin mono-therapy works. For protocols optimising for GH-axis effect, stacking is standard.
Side effects and tolerability#
At typical doses, Ipamorelin's side-effect profile is unusually clean:
- Transient mild hunger — direct ghrelin receptor activation includes some appetite signal, though much less than GHRP-6
- Mild injection-site irritation — common across peptide injections
- Brief light-headed or flushed sensation after dosing (particularly at higher doses)
- Mild transient water retention in the first 1–2 weeks of a cycle
Ipamorelin does not meaningfully elevate:
- Cortisol
- Prolactin
- Aldosterone
- Blood pressure
The side-effect pattern that occurs with GHRP-2 and GHRP-6 — aggressive appetite, mood changes, sustained elevated cortisol — is not part of Ipamorelin's profile at research-use doses.
Regulatory status#
Ipamorelin is not approved as a medicine in the US, EU, or Norway. Legemiddelverket has not authorised Ipamorelin for any indication. Research-use access only.
Klarovel stocks Ipamorelin in multiple formats:
- Ipamorelin standalone: pen (10 mg) and vial (10 mg)
- CJC-1295 + Ipamorelin blend: pen (5 mg + 10 mg) and vial (5 mg + 5 mg)
For most research protocols, the blend is the starting point. Standalone Ipamorelin is useful for protocols that already have a separate GHRH analogue (e.g., Tesamorelin + Ipamorelin rather than CJC + Ipamorelin).
The practical framework#
Three questions filter the Ipamorelin decision:
- What's the goal? GH-axis effects (sleep, recovery, body composition) → Ipamorelin in combination with a GHRH analogue. Single-mechanism support without stacking complexity → Ipamorelin alone at 200 mcg, 1× daily before bed.
- What's the bloodwork baseline? IGF-1, TSH, fasting glucose, and HbA1c at baseline, repeated at 4–6 weeks. Klarovel's questionnaire builds the schedule.
- What's the stack partner? CJC-1295 (no DAC) is the most-used partner. Tesamorelin is an alternative for protocols that prefer an FDA-approved GHRH analogue backdrop (though Tesamorelin is approved for HIV-associated lipodystrophy, not general GH-axis use).
For the stack protocol, see CJC-1295 + Ipamorelin stack. For the reconstitution mechanics, see the reconstitution guide. For dose math, the peptide calculator handles any vial size.
Ipamorelin is the cleanest way to generate amplified GH pulses without the side-effect noise of older GHRPs. It doesn't do anything anabolic-steroid-dramatic, but it does exactly what it's designed to do: trigger cleaner, more selective GH release. That's the point.
Keep reading
Selank Peptide: Russian-Approved, Not FDA-Authorized
Selank peptide is a Russian-approved anxiolytic that modulates GABA-A and enkephalins. The mechanism, the 62-patient trial, and 2026 regulatory reality.
Semax Peptide: Approved in Russia, Unscheduled in the US
Semax peptide is a Russian-approved nootropic that raises BDNF and shows neuroprotective effects after stroke. The science and the 2026 regulatory reality.
Cognitive peptides: promise, evidence, and a retraction
Research-first walkthrough of cognitive peptides, what Semax, Selank, and DSIP actually do, which claims don't hold up, and what to watch in 2026.